
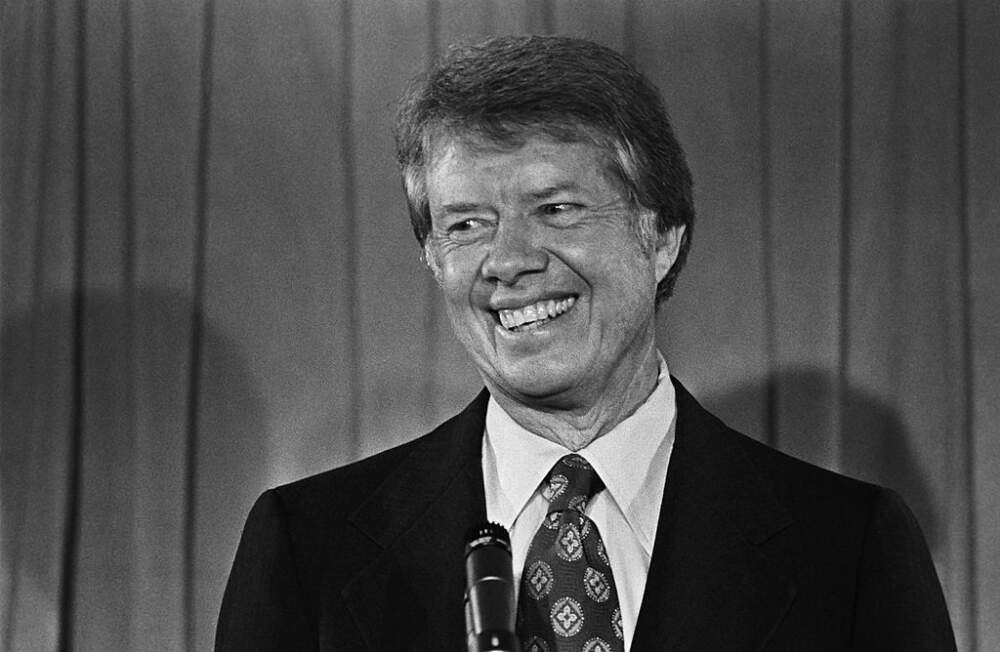
a Jimmy in 1976
Gerald Ford was a pretty decent guy. I would have been fine with him continuing as our president back in the mid-’70s. But he never had a chance of getting my vote in 1976. That’s because he was up against Jimmy Carter.
I had voted for the first time in 1972, and I had a terrible time getting the job done. I must have been in that booth — and we had actual booths back in those days — at least 15 minutes. The holdup was voting for president. I didn’t think much of McGovern. He had run a lame campaign. I was still mad at him for dumping Eagleton. Eagleton had actually been treated for his mental problem. Think what a comfort that would be to us today as we look forward to the inauguration in the coming month.
Mostly, I thought McGovern’s blundering incompetence was an indicator he’d be terrible at the job. Meanwhile, I knew Nixon at least knew how to do the job — but I didn’t trust him one bit. I was sure, even at that early point in the investigations, that he was involved in Watergate. Fortunately, there was a solution — I was sure McGovern was going to lose. So I voted for him, as a protest vote against Nixon. I suppose I finally pulled that lever just as the election volunteers were contemplating sending a search party in after me.
I was happy to have no such problem in ’76. I was for Jimmy all the way. I liked everthing about the guy, mainly that he was different. No, and not “different” like the excuse people use today. He was different in that he was not a crook like Nixon, and a more inspirational figure than poor Ford. And I’m not going simply by the influence of that new show, SNL — which had told me Ford was a klutz, and Carter was the coolest presidential candidate ever — a guy who could, if called upon, talk you down from a bum trip on Orange Sunshine (the cure involved listening to the Allman Brothers).
And it was more than the fact that he had that million-watt smile, which made us feel like everything was going to be fine. Jimmy was here, and we were done with all the crap the country had just been through.
There were more serious reasons. I liked what I had read about what he had done as governor of Georgia. I liked how that might translate into performance as president.
I liked the fact that he was a smart guy — one of Admiral Rickover’s nuclear Navy whiz kids. And he spoke to us as thought he thought we had brains, as well. He leveled with people, even if it set him up for embarrassment, such as when he told Playboy that he had “lusted in his heart” after women other than his wife — and everyone mocked him. At the very peak — or perhaps I should say nadir — of the sexual revolution, he dared to speak of right and wrong, and admit his own failings.
He dared to speak of God, and inspire us by living his life as a man who loved God, and wanted to live according to the wisdom that faith brought him.
I was a copyeditor at The Jackson (Tenn.) Sun at that early point in my career, fresh out of school. I had just joined the paper in the fall of ’75. I was frustrated not getting to write, and looked for anything that could add that enrichment to my dull routine. I volunteered to review books, and our managing editor — who was also our book editor, because that was something he loved — funneled to me any books about this exciting novelty, Jimmy Carter, who had just burst upon the national scene. That fed my enthusiasm.
Being a copyeditor, a desk man, I understood that reporters couldn’t go around with candidates’ bumper stickers on their cars, but cloistered as I was in the newsroom, I saw myself as an exception. And I really liked his green-and-white sticker scheme — a departure from all the blue and red I’d seen in my life, signifying that Jimmy, too, was a departure, and a welcome one. So I put one on the bumper of my orange Chevy Vega.
Probably the clearest (and least relevant, I realize) memory I have of that sticker was on one of my volunteer writing assigments. One weekend I went to Memphis for a book fair, attended by a number of prominent writers of that moment. The organizers set me up to take Mary Hemingway (How It Was) to lunch, and asked me if I’d pick up historian John Toland at the airport. I did so, but as I had not read his new biography of Hitler, we didn’t have much to talk about — except Jimmy Carter. He liked him, too, and therefore liked my sticker. He went back to my bmper and autographed it when I dropped him off at the hotel. By the way, I later read his book, and I recommend it. I learned a lot from it.
Early in the campaign, I got a chance to meet Carter — by, of course, volunteering to go cover a campaign event in Memphis. Since I was there in a journalistic capacity, I knew I wasn’t there to make like a fan. But I did shake his hand. I remember debating with myself whether that was OK, and I think I eventually decided it was. At least, I hope I decided that. It would pain me to realize I passed up that opportunity.
I remained a huge fan for the rest of his life. And it affected me. In the ’90s, I would become president of the board of our local chapter of Habitat for Humanity. That was totally due to Jimmy Carter.
At this point I should probably be running over things he did in office and analyzing them in detail. But while I thought Jimmy did a great job, that’s not why I was such an admirer. I liked and respected Jimmy Carter because he was the best human being to become president of the United States in my lifetime.
And now I thank God for letting him stick around here with us for as long as He did…



